From Variolation to Jenner: The Origins of Preventive Immunization
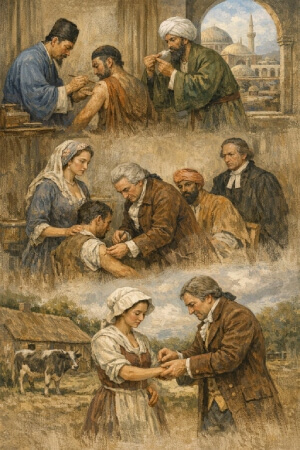
Long before Edward Jenner conducted his famous experiment in 1796, communities across Asia, Africa, and the Ottoman Empire had already developed a crude but functional method of disease prevention known as variolation. The practice involved deliberately introducing material from smallpox pustules into the skin of a healthy person, typically through a small incision or by inhaling dried scabs. Survivors of this controlled exposure generally acquired lasting immunity. Chinese physicians documented the technique as early as the 10th century, and by the 17th century it had spread widely across the Middle East.
Variolation reached Europe largely through the advocacy of Lady Mary Wortley Montagu, who witnessed the practice in Constantinople around 1717 and subsequently had her own children inoculated. Adoption was uneven and contentious. Many physicians remained skeptical, and religious objections ran deep - some argued that deliberately inducing illness interfered with divine providence. The method also carried real risk. Roughly 2 percent of those variolated died from the procedure itself.
Jenner's contribution was to replace that risk with something far safer. Observing that milkmaids who contracted cowpox rarely developed smallpox, he inoculated eight-year-old James Phipps with cowpox material in May 1796, then exposed the boy to smallpox. Phipps showed no infection. The conceptual shift was significant: immunity could be conferred through a related but far milder pathogen. Jenner coined the term "vaccination" from the Latin vacca, meaning cow, and in doing so, laid the intellectual foundation for an entirely new branch of preventive medicine.
Scientific Breakthroughs and the Rise of Modern Vaccines
The germ theory, introduced by Louis Pasteur through the 1860s and 1870s, had something vaccine initiators like Jenner did not have: the germ theory supplied a framework for making sense of vaccines. Once diseases could be pinpointed in microorganisms, the antidote could directly target them and a great sigh of moral and social relief could escape from a civilization that had armed against disease up to that point empirically.
Variolation, invented for a time by Edward Jenner for Small Pox virus, was practically undecided as to whether there was a qualitative essence in the process capable of informing germ physiological mechanisms or a causal physiology. Some few guessed at the truth. The production of antibodies, however, isn't directly in their faces as a reality; what was important then was only to get results.
Pasteur's own experiments were getting successful from attenuated bacterial cultures; thus, vaccines against chicken cholera and anthrax could be made. However, the climax of Pasteur's success was the prophylaxis of rabies, in 1885. When Camille Pelletan first operated on a nine-year-old Joseph Meister against rabies, it was the premier time in the history of medical science that a vaccine had been developed for a viral infection. Owing to these stakes and bright spectacle of this particular case, a change in public opinion against vaccination occurred.
By the early twentieth century, diphtheria antitoxin and the BCG tuberculosis vaccine had entered clinical use, and the 1920s saw the development of toxoid-based vaccines against tetanus and pertussis. Inactivated whole-cell preparations expanded the toolkit further. Each new vaccine reduced mortality in populations that had previously accepted childhood deaths from these diseases as inevitable.
Polio changed everything again. Jonas Salk's inactivated vaccine, licensed in 1955, and Albert Sabin's oral attenuated version, widely deployed through the 1960s, demonstrated that mass immunization campaigns could suppress a feared disease across entire continents. Measles vaccination followed in 1963. These milestones collectively pushed governments to build formal regulatory agencies, national surveillance systems, and cold-chain infrastructure capable of delivering vaccines at scale.
How Vaccination Reshaped Global Health Systems and Population Outcomes
Few public health achievements carry the weight of what happened on May 8, 1980, when the World Health Assembly formally declared smallpox eradicated. The disease had killed an estimated 300 million people in the twentieth century alone. Its elimination through a coordinated global vaccination campaign remains the single most consequential outcome in the history of immunization, and it established a template for every major disease control effort that followed.
The smallpox campaign demonstrated that herd immunity, achieved at sufficient population coverage, could interrupt transmission entirely. When roughly 80 to 85 percent of a population is immunized against a pathogen, susceptible individuals gain indirect protection because the chain of infection cannot sustain itself. Polio eradication efforts applied this same logic. By 2023, wild poliovirus transmission had been interrupted in all but two countries, Afghanistan and Pakistan, reducing annual paralysis cases from an estimated 350,000 in 1988 to single digits.
Falling child mortality rates across the twentieth century correlate strongly with expanded immunization coverage. Measles vaccines alone are estimated to have prevented over 56 million deaths between 2000 and 2021, according to WHO data. Hepatitis B vaccination, introduced into national programs from the 1980s onward, has measurably reduced rates of chronic liver disease and hepatocellular carcinoma in populations with high endemic burden.
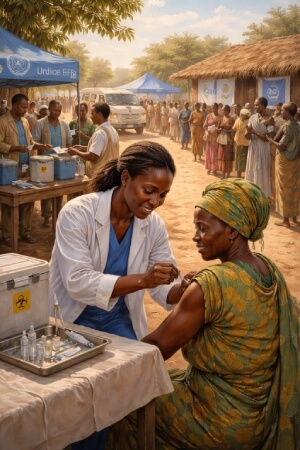
Immunization programs also strengthened primary care infrastructure. Delivery networks built for vaccines became platforms for maternal health services, nutrition interventions, and disease surveillance. Institutions like WHO, UNICEF, and Gavi, the Vaccine Alliance, have financed and coordinated coverage in low-income settings, yet access gaps persist. High-income countries routinely achieve coverage above 95 percent; many low-income nations remain well below 70 percent, constrained by cold-chain failures, supply shortages, and underfunded health systems.
Why Vaccination Remains a Defining Global Health Challenge
Science by itself has not sufficed. Despite a decade-old scientific consensus against the controversies damaging vaccine uptake, these outbreaks still hold down measles in Europe and polio in parts of Asia. Human, rather than scientific, barriers have become the blocks today. Vaccine hesitancy-on account of misinformation-continues to pave the way for low uptake rates, even after explicitly debunked claims about MMR causing autism. Wars accentuate inaccessibility by breaking supply lines and grinding healthcare systems in countries like Yemen and DR Congo. Cold storage capacity is restricted by such basic infrastructure inadequacies. While shortfalls in financing limit the coverage. The COVID-19 pandemic taught us the necessity to innovate speedily, exposing at once the inequalities in access between the affluent and poor countries. Moving forward, most efforts should be directed toward the incentivization of the creation of fair and efficient distribution systems.
“Let food be thy medicine and medicine be thy food.” – Hippocrates
— AncestralHealth☀️ (@AncestralHealtx) November 27, 2025
We took this wisdom, ignored it, and replaced real food with seed oils, sugary junk and pills for every symptom. Your grandparents understood this better than most doctors today: fix your food, and half your… pic.twitter.com/mcGdcHFTRi